status●

Pijn - zenuwblokken Kennisonderwerp
Zie ook:
https://www.nvsha.nl/files/13725/Locoregionale%20anesthesie%201.pdf- n. medianus, n.radialis, n. ulnaris
- n. saphenus, n. peroneus profundus, n. peroneus superficialis, n. suralis, n. tibialis posterior
- Gelaat, oor, mond, n. femoralis en n. pudendus
Polsblok / handblok / wrist block
- Verdoven n. medianus, n. ulnaris, n. radialis (indien wens dorsale zijde verdoven)
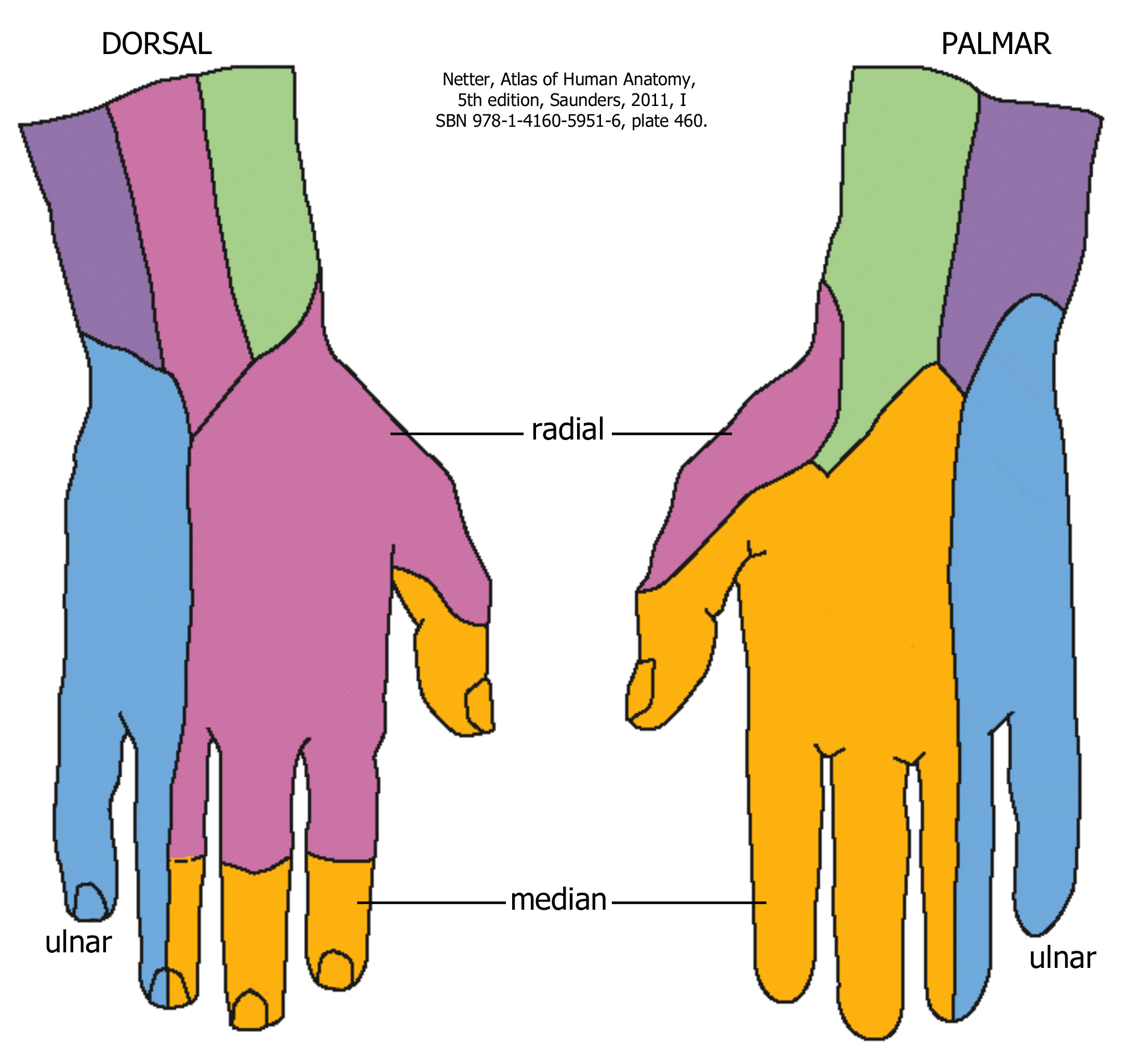
- N. medianus
- Anatomy: At the wrist the median nerve lies between the palmaris longus (PL) and flexor carpi radialis (FCR) tendons. If the PL is absent (15% of the population), the landmark for injection is just medial to the FCR tendon.
- Procedure
1. Have the patient flex the wrist. The FCR and PL (if present) become noticeable in the distal forearm; the FCR is the more lateral of the two tendons.
2. Insert the needle just proximal to the wrist crease and medial to the FCR tendon.
3. Draw back on the syringe and slowly inject 3–5 ml of anesthetic in the tis- sues deep to the skin.
4. If the patient describes minor tingling, the needle is in the proper position. If the patient describes electric shocks or severe pain, the needle may be in the nerve. Stop injecting the anesthetic, and back the needle out a few mm before continuing to inject the anesthetic solution. Do not inject the anesthetic directly into the nerve
- N. ulnaris
- Anatomy: At the wrist, the ulnar nerve lies with the ulnar artery lateral to the flexor carpi ulnaris (FCU) tendon. The artery is lateral to the nerve.
- Procedure
1. Have the patient flex the wrist. The FCU is palpable along the medial edge of the distal forearm.
2. Insert the needle just proximal to the wrist crease and just lateral to the FCU tendon.
3. Draw back on the syringe before injecting the anesthetic to ensure that the needle is not in the ulnar artery. If blood is drawn back, remove the needle and hold pressure over the area for several minutes.
4. Slowly inject 1–2 ml of local anesthetic.
5. To block the nerve branch that supplies sensation to the dorsal aspect of the hand, inject 1 ml of local anesthetic subcutaneously in the tissues overlying the ulnar nerve.
6. Advance the needle onto the dorsum of the wrist, and inject another 3–4 ml. Go about halfway around the wrist on the dorsal surface.
- N. radialis (ramus supercialis)
- Anatomy: The superficial branch of the radial nerve often has several branches traveling in the tissues of the dorsolateral surface of the distal forearm and wrist.
- Procedure
1. Feel for the radial artery pulse in the distal forearm, approximately 2 cm proximal to the wrist crease.
2. Insert the needle laterally to the point where you feel the pulse, and inject 1–2 ml of local anesthetic subcutaneously. Draw back on the syringe before injection.
3. Advance the needle into the tissues on the dorsum of the distal forearm.
4. Inject an additional 3–4 ml of solution halfway around the dorsal surface of the wrist. - Bij toucheren zenuw, mogelijk om tinteling te voelen
Elleboogblokken[1]
- The median nerve may be blocked as it courses posteromedial to the brachial artery superior to the antecubital crease. The nerve is typically blocked using 5 to 10 mL of local anesthetic injected slightly superior to a line connecting the epicondyles. This block can be accomplished using a blind, landmark-based technique, by eliciting paresthesias, or by using a nerve stimulator.
- The radial nerve can be blocked 3 to 4 cm above the lateral epicondyle, close to the distal head of the humerus. After the lateral intramuscular septum has been pierced, paresthesias or a nerve stimulator can be used to localize the nerve. An injection of 5 to 10 mL of local anesthetic will provide an adequate nerve block in this location.
- The ulnar nerve is usually blocked as it runs behind the medial epicondyle. Injection of 3 to 5 mL of local anesthetic is made between the olecranon and the medial epicondyle. Caution must be used to avoid compressing the nerve, because it runs near the bony landmarks
Pudendal block
Genicularis block
- Echogeleid

Overig
- https://lacerationrepair.com/other-topics/blocks/
- Lokale anesthesie in de onderkaak: https://link.springer.com/chapter/10.1007/978-90-368-0231-4_6
- Oogbolanesthesie: retrobulbair blok link
- Sodium bicarbonate increases the pH of the anesthetic solution, shifting the anesthetic agent bupivacaine to its noncationic form that more readily diffuses into surrounding nerves.[2]
Echogeleide blokken
Fenoliseren
Fenol 6-10% (10% het best, moeilijk te krijgen, vraag apotheek AMC)Alcohol 96%
Alleen indien motorische functie niet (meer) nodig
Werkt ca 1 maand voor pijn